Health Insurance Fund Overspending: 'Collapse' before any 'firefighting' measures are taken.
(Baonghean) - The phenomenon of exploiting the health insurance fund has existed for a long time, but only when Vietnam Social Security announced that Nghe An ranked second nationwide in health insurance fund overspending did the relevant parties frantically search for the causes and clarify responsibilities.
Lesson 1:"Going to the hospital with your health insurance card is as easy as... going to the market."
It's no surprise that it exceeded the budget.
In 2016, two new circulars related to health insurance-covered medical examination and treatment services came into effect: Circular 40/2015/TT-BYT regulating initial registration for health insurance-covered medical examination and treatment and referral for health insurance-covered medical examination and treatment, and Circular 37 (jointly) unifying the prices of health insurance-covered medical examination and treatment services among hospitals of the same category nationwide.
 |
| In the first six months of 2016, Nghe An's health insurance fund spent 1,200 billion VND, a 60% increase compared to the same period in 2015. (Illustrative image) |
While Circular 40, also known as the "inter-provincial" circular (effective from January 1, 2016), introduced new prices for medical services, including additional costs such as salaries and special allowances (implementation phased from March 1, 2016). With these changes, Vietnam Social Security (BHXH Vietnam) predicted an increase in medical examination and treatment costs (excluding the impact of the new prices) of approximately 15% compared to 2015. However, by the end of the first six months of 2016, the average increase nationwide had reached 25% based on the old prices and 40% based on the new prices, far exceeding the forecast. It is estimated that 37 provinces nationwide exceeded their allocated budgets by approximately 3,400 billion VND. Nghe An ranks second nationwide in exceeding the allocated budget (351 billion VND), only after Thanh Hoa (the two provinces with the largest populations in the country).
According to a report by the Nghe An Social Insurance Agency, in the first six months of 2016, expenditures from the province's health insurance fund reached nearly 1,200 billion VND, an increase of nearly 60% compared to the same period last year. Regarding the budget overrun, the Nghe An Social Insurance Agency attributed three objective reasons:Increase in medical service prices according to Circular 37.,Streamline medical examination and treatment services according to Circular 40 and increase the number of health insurance cards..
Besides the two reasons predicted by Vietnam Social Security, the increase in the number of health insurance cards leading to increased spending was explained by Mr. Pham Gia Van, Deputy Director of the Provincial Social Security Office: In Nghe An, there are currently about 2.4 million people participating in health insurance, but only 300,000 people pay at the highest rate (4.5% of monthly salary), while the rest are those who pay at low rates, policy beneficiaries (the poor, war veterans, children). However, this group has a high demand for medical examination and treatment and enjoys high benefits, so their participation in health insurance will contribute to increasing the fund's expenditure.
However, do the aforementioned objective reasons explain the enormous overspending figure, placing Nghe An in second place in a worrying ranking? Nghe An Social Insurance stated that the 351 billion VND overspending figure is only the total amount of payment requests from medical facilities; the exact amount paid or disbursed is still under review and no specific conclusion has been reached.
Not yet ready to implement the new Circular
With Circular 40, patients with health insurance cards have the right to receive initial medical examination and treatment at district-level hospitals within the same province. Due to this wider range of choices, patients tend to seek treatment at district-level hospitals instead of through commune health stations as before. According to statistics, the number of patient visits to commune health stations in Nghe An province in the first six months of the year decreased by 195,403 visits (30.34%). As a result, the estimated increase in health insurance expenditure is over 27 billion VND, because the average cost of medical examination and treatment at the district level is approximately 215,550 VND higher per visit than at the commune level.
 |
| Patients wait for their turn to be examined and treated at Vinh City General Hospital - one of the medical facilities that reported exceeding its budget by over 36 billion VND in the first six months of the year. |
The integrated healthcare system also complicates management, as patients can choose any healthcare facility within the same network instead of being tied to their initial registered healthcare facility. In fact, the phenomenon of patients using their health insurance cards to visit and receive medication at multiple facilities within a short period, or even returning to the same healthcare facility, has been observed.
To monitor and mitigate this situation, in June 2016, Vietnam Social Security launched the health insurance claims information system. The system is connected to medical facilities nationwide and is continuously updated. When a patient completes the registration process and enters their health insurance card number, the system provides information about their medical history, thereby detecting any abnormalities.
However, regarding the previous reports about patients successfully accessing numerous medical facilities with their health insurance cards in a short period, the Nghe An Social Insurance agency explained that the system provided only stores data, while the software for managing and entering data varies depending on each medical facility. To date (almost a year after Circular 40 came into effect), the installation and use of the management and data entry software is still incomplete, and even the list of services and techniques is not yet synchronized, hindering the monitoring of medical examination and treatment.
According to observations by a reporter from Nghe An Newspaper at a medical facility in the province, the screen of this supposedly incomplete software still displays the patient's medical history after entering their card number. So, is the fact that patients with the same symptoms can pass through medical facilities in a short period of time truly due to objective reasons?
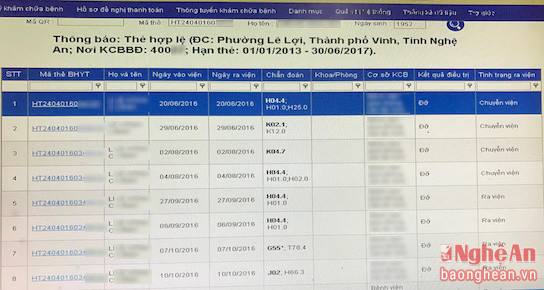 |
| Screenshot of the software at a hospital in the province. The patient's medical history is displayed in considerable detail after entering the patient's health insurance card number. |
Another problem that arose during the implementation of Circular 40 was the ranking of non-public medical facilities. According to the leaders of the Department of Health and Social Insurance of Nghe An province, there are no criteria to classify private medical facilities, yet health insurance payments are linked to their ranking (level). To be able to pay health insurance at private facilities, there is no other way than to allow these facilities to "temporarily" receive payments equivalent to those of ranked public facilities. This explains why private hospitals in Nghe An, which before 2014 received payments equivalent to level IV facilities (commune health stations), were "upgraded" to level II (provincial level) in 2014, and then "dropped" to level III (district level) at the end of 2015. The level of health insurance coverage for medical services in the non-public sector fluctuates accordingly, even though the investment in equipment and facilities in many private establishments is considered to be significantly greater than that of the public sector.
This raises the question: Is there discrimination or inequality between the public and private healthcare systems? Why can't the criteria for evaluating and ranking public hospitals be applied to private hospitals? Leaving aside the rights and responsibilities involved in social welfare mechanisms and policies, the lack of uniformity in standards and assessments will create loopholes in the management of healthcare service quality, impacting social security.
Management "collapses".
In response to the overspending of the health insurance fund and signs of fraudulent activity, the Vietnam Social Security (BHXH) issued Official Letter No. 3358/BHXH-CSYT on rectifying health insurance claims assessment in the last six months of 2016 to its affiliated agencies. The letter emphasized that the abuse and fraudulent activity of the health insurance fund for medical examination and treatment is on the rise at medical facilities, leading to overspending of the health insurance fund in many localities during the first six months of 2016.
The Vietnam Social Security (BHXH Vietnam) requires its affiliated agencies to fully analyze and assess the rate of increase in costs and the imbalance of the health insurance fund for medical examination and treatment in the first six months of 2016, and forecast for the whole year 2016; re-evaluate all health insurance medical examination and treatment costs in the first six months of 2016; strengthen cost control and combat abuse of the health insurance fund for medical examination and treatment…
At the same time, the directive also instructed subordinate agencies to coordinate with the Department of Health to inspect all medical facilities showing signs of abusing funds; after inspection, resolutely recover medical expenses used improperly; in cases of major and systemic violations, transfer the files to the police for investigation…
Following directives from the Vietnam Social Security, the provincial Social Security office, together with the Department of Health, established three inspection teams to examine medical facilities; and coordinated with PC46 of the Provincial Police to investigate, verify, and handle cases involving units suspected of abusing or profiting from the health insurance fund for medical examination and treatment. The provincial Social Security office also reviewed the balance of the health insurance fund for medical examination and treatment in the first six months of the year at medical facilities that experienced sudden "fund overruns".
Furthermore, the agency has taken drastic measures, modifying payment contracts with facilities exhibiting signs of fund abuse; establishing technical barriers to limit the widespread prescription of high-tech tests and services; and adjusting the average cost per person to control healthcare spending. However, these solutions can only provide temporary, unsustainable reductions in fund expenditures. Moreover, with the integration of district-level hospitals within the province, is managing and allocating funds to each hospital based on the number of registered health insurance cards still appropriate?
It's necessary to acknowledge the reality: Streamlining healthcare services means improving the quality of healthcare that people receive, so increased spending is an inevitable consequence. The important thing here is how the Social Insurance agency confronts this change and chooses solutions to regulate and maintain this crucial social welfare mechanism.
Cutting spending on healthcare services or increasing revenue by expanding coverage and raising health insurance premiums – these seemingly contradictory solutions need to be implemented harmoniously, with a clear roadmap and comprehensive monitoring mechanisms to ensure both the rights of citizens and the stability of welfare policies and the healthcare system. We shouldn't wait until things collapse before resorting to sudden, sometimes extreme, firefighting measures.
Reporters

