Drugs that are toxic to the liver.
Most drugs, once in the body, are metabolized in the liver before being excreted via the bile ducts or kidneys. Normally, drugs introduced into the body are non-toxic, but after being metabolized in the liver, some drugs become toxic to the liver itself.
Drugs can cause liver toxicity at varying degrees, from mild to severe necrosis; the disease can be acute or chronic. Symptoms typically appear within 5-90 days of drug use, ranging from loss of appetite and fatigue to jaundice, yellow urine, liver pain, subcutaneous bleeding, and even gastrointestinal bleeding, hepatic coma, and severe liver failure leading to death. With the introduction of many new drugs, the list of drugs that cause liver toxicity is growing longer, including groups such as analgesics, antipyretics, antiviral drugs, and tuberculosis medications.
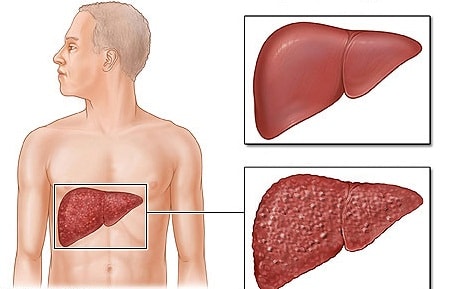 |
| Some medications are highly toxic to the liver, causing chronic liver diseases. |
Antiretroviral drugs
Most antiretroviral drugs inhibit reverse transcriptase or protease, causing hepatitis. Liver damage varies widely from fatty liver to acute hepatitis, and disease progression can be fatal. The mechanisms of toxicity are diverse, either due to the formation of reactive metabolites and inhibition of metabolism in the granular bodies of the liver, or by reactivating hepatitis B and C viral infections.
Paracetamol pain reliever and fever reducer
This is a commonly used medication for treating fever. The drug is toxic to the liver depending on the dose used. When treating patients, it is important to consider the dose that causes liver toxicity. At doses less than 2-3g/day, paracetamol is considered safe and tolerable. Oral doses greater than 10-15g can lead to severe liver damage, often fatal; this dose is typically used in cases of suicide. Paracetamol-induced liver damage is a common form of drug-induced liver disease. In alcoholics, even the usual therapeutic dose of paracetamol can be toxic to the liver; therefore, caution should be exercised when using paracetamol in alcoholics, and it should not be taken with alcoholic beverages.
Anti-tuberculosis drugs
Drugs such as isoniazid, rifampicin, streptomycin, and especially isoniazid (INH) have been the primary treatment for tuberculosis since the mid-20th century. Elevated liver enzymes occur a few weeks after starting tuberculosis treatment in approximately 10-20% of patients using INH. This elevation is usually moderate and not associated with signs or symptoms of liver disease. Many patients with elevated liver enzymes tolerate continued INH use and may subsequently return to near-normal levels. If elevated liver enzymes occur, discontinuing INH will return them to normal within 1-4 weeks. However, a small number of patients using INH may experience acute liver failure (occurring in about 0.1-2% of patients). Patients over 50 years of age are at higher risk of hepatitis when using INH, while liver damage is less common in children. Female patients are more affected than male patients. During treatment, close monitoring is necessary to detect INH-induced hepatitis so that treatment can be stopped promptly, avoiding severe liver damage.
Vitamin A
Excessive vitamin A intake can cause dose-dependent liver toxicity, potentially leading to cirrhosis. Regularly taking large doses of vitamin A (>25,000 units/day) can cause chronic toxicity and liver damage. Liver damage can occur with 15,000-40,000 units/day for a year, but higher doses can cause toxicity within months. The severity of liver damage depends on the dose and duration of use. Many patients with vitamin A-induced liver disease may not be aware of it until clinicians observe symptoms such as prolonged vitamin A use accompanied by fatty liver disease and portal hypertension. Alcoholics are at even higher risk.
Other drug groups
In addition, several other groups of drugs can also harm the liver, such as antifungal drugs (nystatin, ketoconazole, fuconazole), antithyroid drugs (PTU, MTU), diabetes medications (sulfamides, troglitazone, rosiglitazole), cardiovascular medications (amiodazone, methyldopa, quinidine), and anticonvulsants (phenytoin, carbamazepine)...
Besides the side effects of the medication, we also need to pay attention to several factors that increase the toxicity of drugs to the liver, such as alcohol (alcohol increases the toxicity of most drugs to the liver, including paracetamol and isoniazid); pre-existing liver and biliary diseases (such as chronic hepatitis, cirrhosis, etc.); dosage of the drug (some drugs are safe at low doses but at high doses or in overdose will cause acute liver toxicity); and drug interactions that increase the potential for liver toxicity (the combination of isoniazid with rifampicin will increase the hepatotoxicity of rifampicin).
Therefore, to use medication safely, patients need to strictly follow the doctor's instructions and orders, and should not abuse or self-medicate. If symptoms such as loss of appetite, aversion to fatty foods, dark urine, or pain in the liver area occur while taking medication, they should immediately go to medical facilities for examination, detection, and timely treatment.
According to suckhoevadoisong

